ICSI Treatment in Delhi— Higher IVF Success
Precision micro-injection technology for couples with male-factor infertility, prior IVF failures, or limited egg numbers. Performed by expert embryologists at KIC Delfinium — fertilisation rates of 75–82%.
What Is ICSI — And How Does It Differ from IVF?
For couples struggling with male-factor infertility, previous IVF failures, or limited egg numbers, Intracytoplasmic Sperm Injection (ICSI) represents a pivotal advance in assisted reproduction. At Kiran Infertility Centre (KIC Delfinium) Delhi, our embryology team performs ICSI with precision micro-injection technology, achieving outcomes that consistently meet international benchmarks.
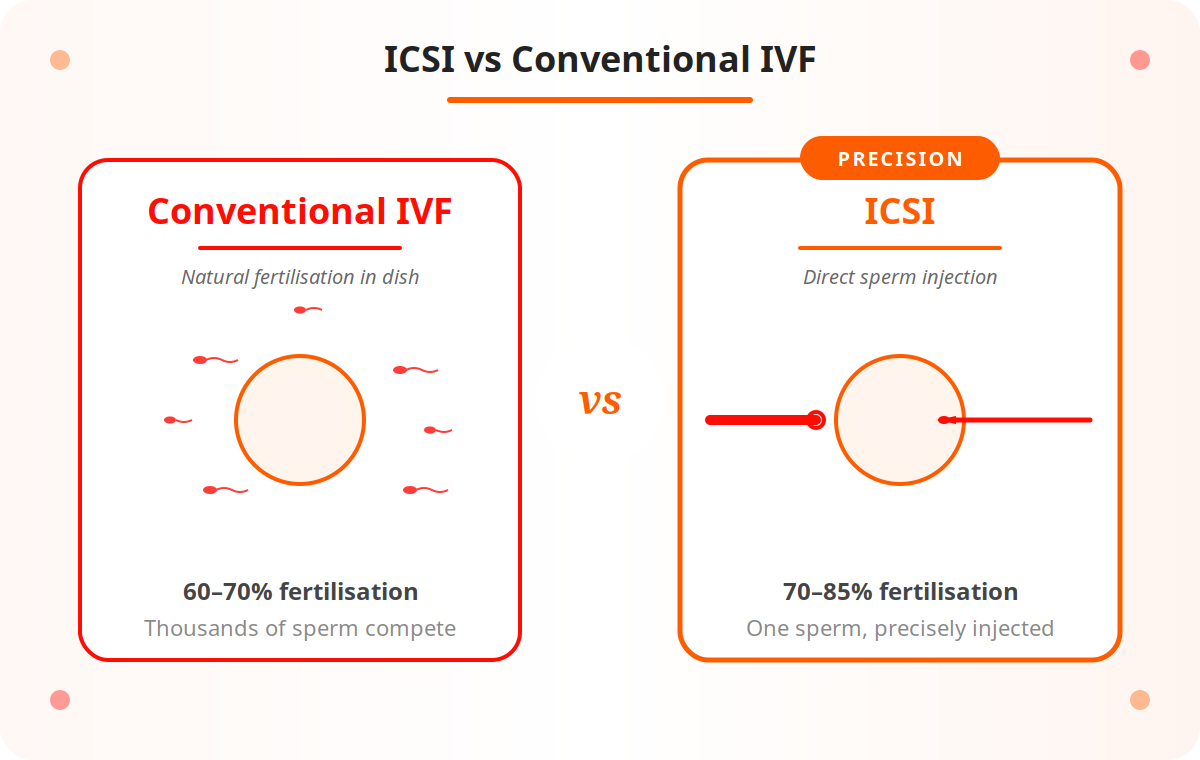
In conventional IVF, thousands of sperm are placed in a dish with an egg and left to fertilise naturally. Success depends on the sperm’s own ability to penetrate the egg’s outer shell. When sperm count, motility, or morphology is severely compromised, natural penetration may not occur — resulting in failed or very low fertilisation.
Using a glass microneedle less than 1 micron in diameter, an embryologist selects a single healthy sperm under high-powered magnification (200–400×) and injects it directly into the egg. The sperm no longer needs to swim or drill — fertilisation is mechanically assisted at the cellular level. The rest of the cycle is identical to standard IVF. ICSI is not a separate treatment; it is a fertilisation method used within an IVF cycle.
The ICSI Procedure Explained
Each ICSI cycle is a precise, multi-stage process performed by our specialist embryology team. The female partner undergoes the same stimulation and retrieval as standard IVF; the difference lies in the laboratory work that follows.
Below is a detailed walkthrough of every stage, from ovarian stimulation through to embryo transfer and the two-week wait.
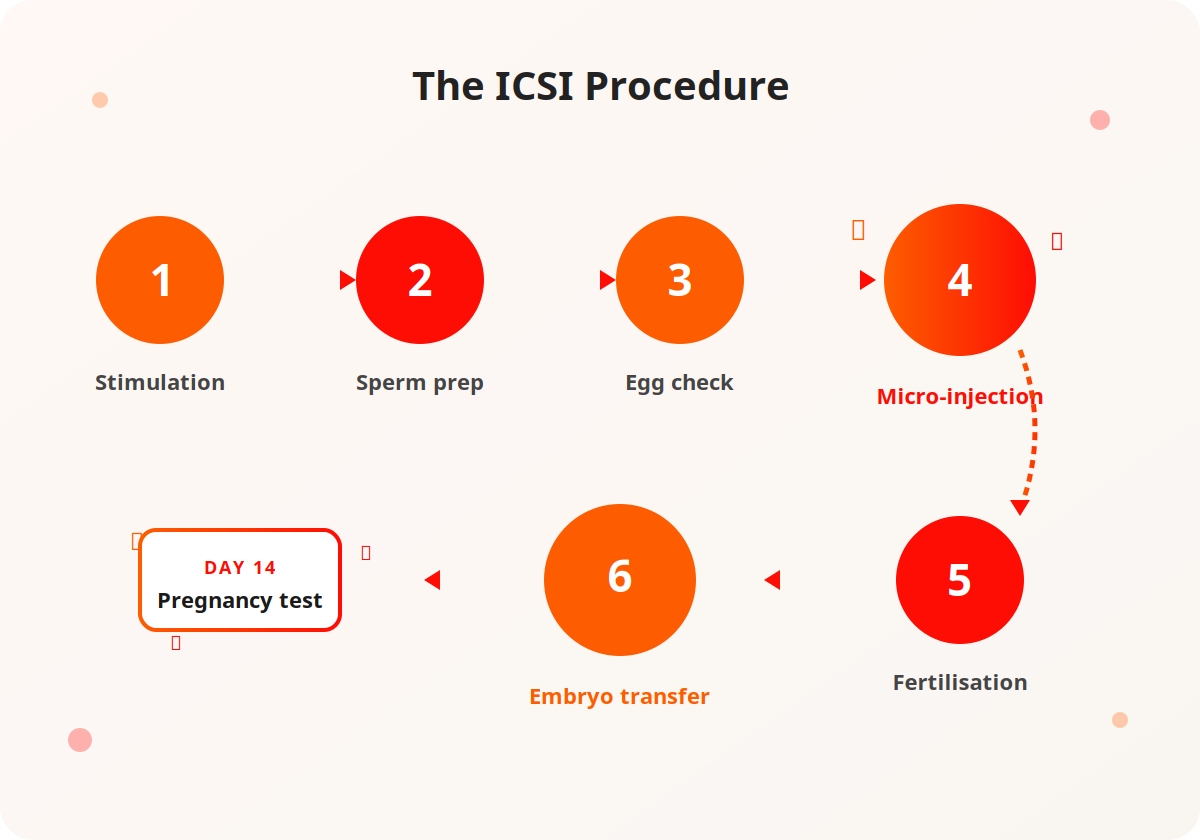
Ovarian Stimulation & Egg Retrieval
10–14 days of hormone injections, monitoring scans, trigger injection, and a minor day-care retrieval under sedation — identical to standard IVF.
Sperm Preparation
The male partner provides a semen sample (or surgically extracted sperm). Embryologists use density gradient centrifugation or swim-up to isolate the highest-quality motile sperm.
Egg Maturity Assessment
Retrieved eggs are examined within 2–4 hours. Only mature MII (metaphase II) eggs are suitable for ICSI. Immature eggs may be cultured further for IVM.
Micro-Injection
Each mature egg is held by a pipette while a single morphologically normal sperm is loaded into the injection needle and precisely injected into the cytoplasm.
Fertilisation Check & Embryo Culture
18 hours after injection, eggs are checked for fertilisation. Successfully fertilised eggs are cultured for 3–5 days. Blastocyst culture (Day 5) is preferred when possible.
Embryo Transfer
The best embryo(s) are transferred to the uterus using a thin catheter under ultrasound guidance. Surplus good-quality embryos are vitrified for future use.
When Is ICSI Recommended?
KIC Delfinium’s fertility specialists recommend ICSI in the following clinical situations.
Severe Male-Factor Infertility
Very low sperm count, poor motility, abnormal morphology, or OAT syndrome. ICSI can achieve fertilisation even with just a few thousand motile sperm per millilitre.
Surgically Retrieved Sperm
When sperm is extracted via PESA or TESA/TESE due to vasectomy, absent vas deferens, or obstructive azoospermia — ICSI is required to fertilise the eggs.
Prior IVF Fertilisation Failure
If a previous conventional IVF cycle produced zero or very low fertilisation (under 30%), ICSI is recommended for subsequent attempts to maximise fertilisation.
Low Egg Numbers
For women with low ovarian reserve or older patients, ICSI ensures every available egg has the highest possible chance of fertilising — no reliance on natural competition.
Frozen Sperm
Cryopreserved sperm (oncofertility banking, donor sperm, stored samples) has reduced post-thaw motility. ICSI is routinely recommended for frozen sperm samples.
ICSI vs Conventional IVF
Clinical pregnancy rates are similar when sperm parameters are normal. ICSI’s key advantage is rescuing fertilisation when conventional IVF would fail.
| Metric | Conventional IVF | ICSI |
|---|---|---|
| Fertilisation rate | 60–70% | 70–85% |
| Compromised sperm | Often fails | Achieves fertilisation |
| Pregnancy < 35 | 40–50% | 40–55% |
| Cost vs base | Base | 10–15% higher |
| Fertilisation failure risk | Higher in male-factor | Significantly reduced |
ICSI Cost at KIC Delfinium Delhi
A fully itemised breakdown so there are no surprises — you receive a personalised cost estimate after your initial assessment.
| Component | Approximate Cost |
|---|---|
| Fertility Assessment & Pre-Treatment Tests | ₹5,000 – ₹8,000 |
| Ovarian Stimulation Medications | ₹50,000 – ₹90,000 |
| Monitoring Scans & Lab Tests | ₹8,000 – ₹12,000 |
| Egg Retrieval + Anaesthesia | ₹30,000 – ₹45,000 |
| ICSI Embryology Lab Charges | ₹20,000 – ₹30,000 |
| Embryo Culture to Blastocyst | ₹10,000 – ₹15,000 |
| Embryo Transfer + Luteal Support | ₹15,000 – ₹25,000 |
| Embryo Vitrification (if surplus) | ₹15,000 – ₹20,000 |
| Total ICSI Cycle | ₹1,50,000 – ₹2,20,000 |
Sperm retrieval procedures (PESA/TESA) are charged separately — ₹15,000–₹35,000 depending on technique. EMI plans available — speak to our patient counsellors.
ICSI vs IMSI vs PICSI
Beyond standard ICSI, KIC Delfinium offers two enhanced sperm-selection techniques for couples with specific challenges.
| Feature | ICSI | IMSI | PICSI |
|---|---|---|---|
| Magnification | 200–400× | 6,000–7,000× | Standard |
| Selection basis | Motility & morphology | Nuclear quality | Hyaluronan binding |
| Best for | Most male-factor cases | High DNA fragmentation | Recurrent miscarriage |
| Additional cost | — | ₹10K – 15K | ₹5K – 8K |
| Evidence level | High | Moderate-high | Moderate |
IMSI uses ultra-high magnification to exclude sperm with nuclear vacuoles invisible under standard ICSI. PICSI selects sperm by their ability to bind hyaluronan — a marker of maturity and DNA integrity. Learn more about IMSI and PICSI.
Risks and Considerations
ICSI has an excellent safety record — one of the most widely performed assisted reproduction techniques worldwide.
OHSS (Hyperstimulation)
A risk in all IVF/ICSI cycles. KIC’s monitoring protocols and dose adjustments keep severe OHSS rates below 1%.
Fertilisation Failure (rare)
Though uncommon (2–5% of cycles), ICSI can still fail to fertilise eggs in cases of severe egg or sperm dysfunction.
Genetic Considerations
In severe male-factor cases, genetic testing (karyotyping, Y-chromosome microdeletion) is recommended before ICSI to avoid transmitting genetic causes of infertility.
Multiple Pregnancy
Transferring more than one embryo increases the chance of twins. KIC follows evidence-based single embryo transfer guidelines where appropriate.
Egg Damage (rare)
Micro-injection can occasionally damage the egg. Experienced embryologists at KIC Delfinium maintain rates well below the 3–5% industry average.
Why Choose KIC Delfinium for ICSI
Outcomes in ICSI depend more on embryology lab quality than any other treatment. Choosing the right team matters.
- Precision micro-injection using glass needles less than 1 micron in diameter under 200–400× magnification
- Expert embryology team with UK-trained leadership and decades of combined experience
- IMSI & PICSI available for couples with DNA fragmentation, recurrent failures, or poor embryo quality
- Below-industry-average egg damage rates — a direct reflection of embryologist skill
- Severe OHSS rate below 1% thanks to careful monitoring and dose adjustments
- Fully itemised cost estimates with EMI options available through healthcare financing partners
Frequently Asked Questions
Honest answers to the questions couples ask most often before starting ICSI.
Is ICSI better than IVF for everyone?
Not necessarily. When sperm parameters are normal, conventional IVF and ICSI produce comparable pregnancy rates. ICSI is specifically superior when male-factor infertility, prior fertilisation failure, or surgically retrieved sperm are involved. Your KIC Delfinium specialist will recommend the right approach for your individual case.
How many ICSI cycles might I need?
Most couples who will succeed with ICSI do so within two to three cycles. The number depends on age, egg quality, embryo development, and endometrial receptivity. KIC Delfinium’s team reviews each cycle thoroughly before planning the next to maximise your chances.
Can ICSI help in cases of azoospermia (zero sperm count)?
Yes. If no sperm are present in the ejaculate, surgical sperm retrieval (PESA or TESA) can obtain sperm directly from the epididymis or testis in many men with obstructive or even non-obstructive azoospermia. These sperm are then used for ICSI.
Is the baby born after ICSI normal and healthy?
Decades of data from millions of ICSI births worldwide confirm that babies conceived via ICSI have no higher risk of birth defects than naturally conceived babies, beyond a marginally increased risk associated with underlying male infertility itself (not the ICSI procedure). Preimplantation Genetic Testing (PGT) can further screen embryos before transfer when indicated.
How long does the ICSI process take from start to pregnancy test?
A complete ICSI cycle — from stimulation start to pregnancy test — takes approximately 5–6 weeks. The stimulation and retrieval phase lasts 2–3 weeks; embryo culture to blastocyst takes 5 days; the transfer cycle (fresh or frozen) adds a further 2–3 weeks.
What is KIC Delfinium Delhi’s ICSI success rate?
KIC Delfinium’s ICSI fertilisation rate is 75–82%, and clinical pregnancy rates (confirmed heartbeat on scan) for women under 35 using their own eggs are in the range of 45–55% per embryo transfer — outcomes consistent with leading IVF centres globally.
Does male age affect ICSI outcomes?
Yes. While men can produce sperm throughout life, sperm quality — including DNA fragmentation — declines with age, particularly after 40–45. Higher sperm DNA fragmentation reduces fertilisation and embryo quality even with ICSI. In such cases, IMSI or PICSI may be added to the protocol.

Begin Your ICSI Journey at KIC Delfinium
Our expert embryologists are ready to help. Book a consultation today — we’ll review your history, recommend the right approach, and give you a transparent cost estimate tailored to your situation.
New Delhi 110049
9 AM – 5 PM